

























Prostatitis is a disease characterized by the presence of inflammation and / or infection localized in the prostate gland.
It can present with a wide range of clinical signs and complaints.
Anatomy
The prostate is a small gland that is part of the male reproductive system and a hormone-dependent organ. Its shape and size have been compared to a large nut. A normal prostate gland weighs about 20 g, has a volume of 15-25 ml and measures 3 cm in length, 4 cm in width and 2 cm in depth.
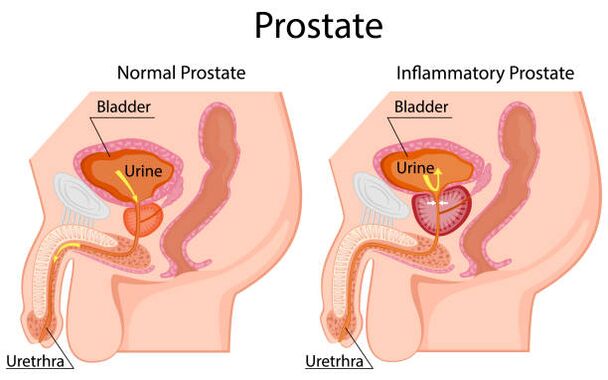
The prostate gland is located in the small pelvis, below the bladder and above the rectum. The urethra, the urethra, passes through the thickness of the gland. The prostate is surrounded by a capsule composed of smooth muscle, collagen, and elastic fibers; covered with three layers of dense connective tissue (fascia) on the anterior, lateral, and posterior surfaces. The posterior surface of the prostate is bounded by the ampulla of the rectum. They are separated by the retrovesical fascia or Denonville fascia, which allows palpation of the posterior surface of the prostate gland.
The prostate gland is approximately 70% glandular tissue and 30% fibromuscular stroma. It is customary for the organ to be divided into 3 zones.
Transition zone.The transition zone accounts for 10% of glandular tissue and 20% of cases of malignant prostate tumors. In this area, one of the main age-related diseases in men is formed - benign prostatic hyperplasia, which can lead to difficulty urinating due to tissue overcrowding.
Central area.The area around the ejaculatory ducts. It consists of glandular tissue, connective tissue and muscle elements. Tumors in this area are extremely rare.
Peripheral area.Covers the back and sides of the prostate gland and contains 70% of glandular tissue. This is an area that is palpable through the rectum and allows the urologist to assess the condition of the prostate gland. Up to 70% of malignant tumors are located precisely in the peripheral area. Therefore, digital colon examination is an important diagnostic method and should be performed in patients over 45 years of age.
Prostate functions:
- production of prostate secretion, which is an integral part of sperm and is involved in the liquefaction of ejaculate, as well as its saturation with nutrients such as various enzymes and vitamins, citric acid, zinc ions, which help to improvesperm movement and activity;
- The prostate contains smooth muscle fibers that help release sperm from the urethra during ejaculation, prevent sperm from entering the bladder, and are involved in the urinary retention mechanism.
Prostatitis, benign prostatic hyperplasia and prostate cancer are the three main prostate diseases.
All three diseases can coexist in the same prostate at the same time. That is, the presence of prostatitis does not exclude the presence of prostate hyperplasia and prostate cancer in the patient and vice versa.
Causes of prostatitis
According to statistics, prostatitis is the most common urological disease - after prostate hyperplasia and prostate cancer - in men under 50 and the third most common in men over 50.
Prostatitis accounts for 6 to 8% of outpatient urological visits.
The most common causative agent of prostatitis is E. coli strains, which are detected in 80% of cases. The rarest pathogens are enterococci, Pseudomonas aeruginosa, Klebsiella and other gram-negative bacteria. The role of sexually transmitted infections (such as chlamydia trachomatis) in prostate inflammation has not yet been clearly defined and is under study. In patients with HIV infection and other severe changes in the immune system, possible causative agents are cytomegalovirus, mycobacterial tuberculosis, fungi, and other rare pathogens. There is evidence to suggest the presence of microorganisms in the prostate gland that are not detected in standard studies, but play a role in the onset of inflammatory changes and the subsequent development of prostate symptoms.
Possible causes of prostatitis are:
- intraprostatic reflux of urine as a result of dysfunctional urination (urine, with certain predisposing factors, can enter the prostate gland through the prostate ducts, causing an inflammatory process);
- unprotected anal sex;
- foreskin narrowing (phimosis);
- autoimmune diseases;
- functional and anatomical changes in the pelvic muscles;
- changes in the central nervous system, including functional and anatomical changes in the brain;
- traumatic and unusual sexual activity;
- psychological factors (in a number of studies, the impact of psychological stress on the onset of chronic prostate symptoms has been proven - in some patients psychosomatic disorders have been diagnosed, in the treatment of which a decrease in prostate symptoms and the likelihood of its recurrence were noted).
Risk factors for prostatitis also include: abstinence or excessive sexual activity, the habit of stopping ejaculation, smoking, working at night, a sedentary lifestyle, inadequate fluid intake and poor diet.
Symptoms
- pain or burning when urinating (dysuria);
- urinary disorders;
- urine stain;
- the appearance of blood in the urine;
- pain in the abdomen, groin or lower back;
- pain in the perineum;
- pain or discomfort in the penis and testicles;
- bleeding pain;
- increased body temperature (with acute bacterial prostate).
Diagnosing
According to the generally known classification of prostatitis NIH (National Institutes of Health of the U. S. B. A. ), there are four categories of diseases, traditionally marked with Roman numerals:
- I - acute bacterial prostatitis;
- II - chronic bacterial prostatitis;
- III - chronic abacterial prostatitis / chronic pelvic pain syndrome (CP / CPPS);
- IIIa - chronic prostatitis / chronic pelvic pain syndrome with signs of inflammation;
- IIIb - chronic prostatitis / chronic pelvic pain syndrome without signs of inflammation;
- IV - chronic asymptomatic (asymptomatic) prostatitis.
Despite the prevalence of prostatitis, acute bacterial prostatitis is not common - 5% of all cases of the disease. But his diagnosis is quite simple, as the picture of the disease is most often highlighted: a man complains of frequent, painful urination, pain in the uterus and perineum. An increase in body temperature is characteristic, and often at high values - less than 39 ° C.
Diagnosis of acute bacterial prostatitis involves a digital examination of the colon (examination of the colon), which involves the sensation (palpation) of the prostate gland with the index finger through the anus (rectum).
Digital colon examination (DRE) is an important diagnostic manipulation if any pathology of the prostate gland is suspected. Therefore, it is advisable that men do not refuse to perform it.
In acute bacterial prostatitis, the prostate when touched is highly painful, edematous, most often enlarged. Ultrasound examination can show not only an increase in the size of the prostate gland, but also foci of purulent union of prostate tissue (abscesses) - but this rarely happens and, as a rule, is a consequence of a running process.
Laboratory diagnosis, first of all, involves a general urine test, in which an increase in the number of leukocytes is observed. Bacteriological culture of urine is recommended. Based on the results of the analysis, it is possible to determine the presence of bacteria and their sensitivity to the antibiotic and, thus, to adjust the prescribed antibiotic therapy. A general blood test is also performed to assess the general condition of the body and its response to the inflammatory process.
Taking prostate secretions for diagnosis in acute prostate is contraindicated due to the increased risk of a life-threatening condition: bacteremia and sepsis. Determination of oncomarker (PSA), its fractions is also not recommended - due to low information content and data distortion on the background of inflammation.
Treatment of prostatitis
Antibiotic therapy is the basic therapy for prostate patients of all categories.
Alpha-blockers are also an effective group of drugs. As a result of their action, the tone of the smooth muscles of the prostate gland, bladder neck and prostate part of the urethra is reduced, thus improving urination and reducing the possibility of urine entering the prostate gland (intraprostatic reflux of urine), ewhich is one of the causes of prostatitis. The most effective and popular drugs are Tamsulosin and Silodosin. They are also widely used to improve urination in patients with prostate hyperplasia.
It is possible to use anti-inflammatory drugs (Diclofenac), which effectively reduce pain and discomfort during urination, reducing prostate swelling and also contribute to some improvement in the quality of urination.
Acute bacterial prostatitis is often a reason for hospitalization in a hospital where antibiotic therapy in the form of intravenous injections is prescribed. After the patient's condition stabilizes, the patient continues to take antibiotics in tablet form for 15 days or more in order to prevent the transition from acute prostatitis to chronic bacterial prostate.
According to statistics, 10% of patients with acute prostate develop chronic bacterial prostate. Another 10% of patients will develop chronic pelvic pain syndrome (chronic prostatitis IIIb) in the future.
How is prostatitis treated in the clinic
Urologists treat prostatitis and other diseases of the genitourinary system, based on international clinical guidelines. This means that they not only use their professional knowledge, but are also guided by scientifically proven and universally accepted methods for diagnosis and therapy.
Our doctors do not prescribe ineffective medications and examinations "just in case", they do not treat non-existent diseases. When making a diagnosis, urologists rely on data obtained from the patient examination, clinical appearance, data of laboratory and instrumental studies. If surgical treatment is required, a surgical operation is performed on the territory of the clinic.